젖 먹는 아기에게 생긴 급성 탈수증, Acute dehydration in breastfeeding infant
1. 체내 수분, 전해질 균형과 탈수
- 신체 총 수분양이 정상보다 적어지는 현상을 ‘탈수’라고 한다.
- 탈수로 생기는 증상이 ‘탈수증’이고,
- 갑자기 생긴 탈수증은 ‘급성 탈수증’,
- 만성으로 생긴 탈수증을 ‘만성 탈수증’이라 한다.
- 탈수증은 신생아들, 영유아들, 학령기 아이들, 사춘기 아이들 등 연령을 가릴 것 없이 누구에게도 생길 수 있다.
- 하지만, 탈수증은 특히 영유아들에게 더 쉽게, 더 심하게 생길 수 있다.
- 다행히도 젖을 먹는 영유아들에게 구토 및, 또는 설사는 잘 생기지 않는다.
-
-
미숙 신생아의 총 체중의 80%,
-
1세 유아의 총 체중의 65%,
-
성인의 총 체중의 60%가 수분이다.
-
- 경구로 섭취한 매일 필요 하는 수분과 K⁺, H⁺, Cl⁻, Na⁺, HCO3⁻ 등 전해질이 위장관 벽 점막층을 통과해 혈액 내로 흡수된다.
- 필요 이상으로 섭취한 수분과 전해질은 소변, 대변, 땀 등을 통해 신체 밖으로 배설된다. 신체 내 총 수분의 양과 총 전해질의 양이 일정하게 유지되고 전해질 평형이 잡힌다.
- 신체 내 수분과 전해질이 필요 이상으로 더 많으면 필요 이상으로 더 많은 수분과 전해질은 피부, 호흡기, 비뇨기, 위장관 등을 통해 몸 밖으로 배출된다.
- 만일 영아가 모유, 인공영양, 이유식, 밥상 음식물을 조금도 먹지도 못하고 마시지도 못하거나, 어떤 병으로 수분과 전해질을 적절히 보충 받지 못할 때는, 신체 내 수분과 전해질을 가능하면 배출시키지 않는다.
- 나트륨이온 (Na+), 칼륨이온 (K+), 클로라이드 이온(Cl-), 중탄산기 이온(HCO3-) 등 체내 전해질과 체내 수분 평형이 일우진다.
- 섭취하는 수분 양이나, 전해질 양보다 수분과 전해질을 어떤 병, 굶음, 그 외 다른 이유로 신체 밖으로 많이 잃을 때 탈수증과 전해질 불균현이 생길 수 있다.
- 탈수되면 신체 내 총 수분의 일부만 잃는 것이 아니라 나트륨 이온, 칼륨 이온, 염소 이온 등 전해질도 잃는다. 그와 동시에 혈액이 산성화가 되든지 알칼리화가 될 수 있다.
- 특히 영아들이나 유아들이 바이러스성 위장염이나 박테리아성 위장염으로 설사, 구토 할 때 심하게 탈수될 수 있다.
- 이때 모유, 인공영양, 이유식 등 어떤 종류의 음식물을 조금도 먹지 못하면 탈수되고 전해질 소실 이 생겨 탈수증과 전해질 불균형이 생길 수 있다.
- 소화가 전혀 되지 않은 음식물, 모유, 또는 인공영양, 일부 소화된 음식물, 혈관 속에서 위장관 벽 점막층을 통해 위장관 속으로 분비된 수분, 전해질, 위장관 벽 점막층에서 분비된 위장액, 췌장액, 담즙 등이 위장관 내에서 섞이게 된다. 위장관 내 혼합물이 된다.
- 위장염을 앓을 때는 위장관 내 혼합물이 위장관 벽 점막층을 통과해 피 속으로 정상적으로 흡수되지 못하고, 소장관 속→대장관 속→항문으로 배설된다. 즉 위장관 내 혼합물이 설사 변으로 된다.
- 구토를 할 때도 상부 위장관 속에 있는 소화가 안 된 음식물과 위액 등이 토해 입 밖으로 나온다.
- 이런 현상을 구토라고 한다.
- 위 내용물이 바로 구토물이다.
- 십이지장관 이하 하부 소장관의 일부가 막히면 먹은 음식물과 위액을 토할 수 있고, 췌장액, 담즙액, 장관 벽 점막층에서 분비된 장액 등이 섞인 “위장관 내 혼합물”을 토할 수 있다.
- 이때 ‘여과성 설사’를 할 수 있다.
- 다시 설명하면, 설사와 구토를 할 때 설사 변이나 구토 물의 대부분은 입으로 마시고 먹은 음식물, 모유, 인공영양, 이유식 등과 위장관 액, 장액, 혈관 속에서 위장관 벽 점막층을 통과해서 나온 체액 등이 혼합된 “위장관 내 혼합물”이다.
- 구토 및, 또는 설사를 할 때 체내 혈액 내 수분과 전해질이 정상 이하로 감소되고 체내의 수분과 전해질의 총량이 감소되면서 탈수가 생기는 것이 보통이다.
- 참고로 설사 및 구토에 따른 생리를 설명한 것이다.
- 설사, 구토를 치료하는데 많은 도움이 될 것이다.(부모도 반의사가 되어야 한다 ―소아가정간호백과-제 9권 소아청소년 소화기 질환- 로타바이러스 위장염, 로타바이러스 감염으로 인한 위장염 참조)

사진 4-157. 설사 변.
소화되지 않은 음식물과 위장관의 점막층을 특히 흡수되지 않은 수분 및 장액이 섞여 묽은 변으로 나오는 것을 설사라고 한다. 장액 속에는 전해질이 들어 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
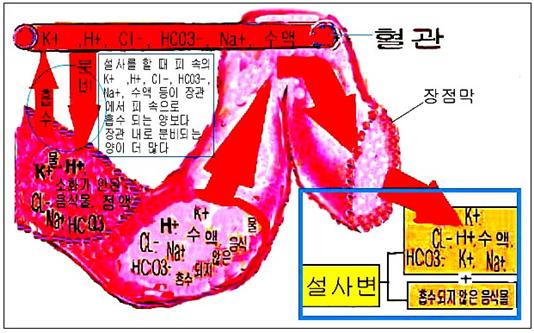
그림 4-33. 위장염 등으로 위장관 벽 점막층이 손상되거나 부어서 설사를 할 때의 전해질과 수분의 이동, 설사 변의 구성. 칼륨 이온(K+), 수소 이온(H+), 염화물 이온(Cl-), 나트륨 이온(Na+), 중탄산기 이온(HCO3-) 등 전해질이 장액, 소화되지 않은 음식물과 섞여 설사 대변으로 정상 이상 배설될 수 있다.
이렇게 본 대변을 설사라고 한다.
갑자기 많이 설사하면 탈수가 되고 전해질도 잃고 전해질 불 균형화가 생기고 혈액의 산성도(pH)도 변화될 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
2. 탈수의 원인
- 모유나 인공영양을 먹는 신생아들이나 영유아들 또는 밥상 음식물을 먹는 영유아들, 학령기 아이들이 아무 병이 없이 한두 끼니를 먹지 않고 굶으면 경미하게 탈수 될 수 있고 탈수증이 생길 수 있다.
- 어떤 병으로 설사나 구토를 하지 않아도 한두 끼니를 굶으면 탈수될 수 있다.
- 간장이나 소금을 과량 섭취했을 때,
- 음식물을 아주 짜게 많이 먹었을 때,
- 어떤 원인으로 구토와 설사를 할 때,
- 설사를 끓인 탈지 우유로 치료 할 때
- 소금 중독 및, 또는 고장성 탈수가 생길 수 있다.
- 위장염으로 생긴 설사나 구토, 집에서 만든 경구용 전해질 용액으로 탈수를 치료할 수 있다.
- 그러나 설사 및, 또는 설사의 치료에 쓸 경구용 전해질 용액을 집에서 만들 때 권장한 양 이상 소금이나 소다의 양을 자칫 잘못해 더 넣거나 덜 넣어 가정 경구용 전해질 용액을 만들거나, 잘못 만든 가정 경구용 전해질 용액을 과량 섭취할 때 소금 중독이나 고장성 탈수가 생길 수 있다.
- 전혀 치료한 적이 없는 1형 당뇨병, 제대로 치료되지 않은 1형 당뇨병, 바이러스성 위장염이나 박테리아성 위장염 등으로 인해 설사 및 구토를 심하게 할 때도 급성 탈수증이 생길 수 있다.
- 드물게 유문협착증으로 구토 할 때도 탈수와 전해질 불균형이 생길 수 있다.
- 그 밖에도 심한 화상, 출혈, 그 외 다른 질병을 앓을 때 음식물을 소량 먹고 수분을 소량 마시면 탈수 될 수 있다.
- 특히 신생아나 영유아가 위장염 등으로 먹지도 마시지도 못하고, 토하고, 설사하고, 열 날 때는 짧은 시간 내 심하게 탈수될 수 있다.
3. 탈수의 증상 징후
표 5-4. 신체 각 기관의 체액의 전해질 성분(pH)과 삼투압
| 혈액이나 체액
전해질의 종류 |
Na+ | K+ | Cl- | HCO3- | pH | 삼투압 |
| 위액 | 50 | 10~15 | 150 | 0 | 1 | 300 |
| 췌장액 | 140 | 5 | 50~100 | 100 | 9 | 300 |
| 담즙 | 130 | 5 | 100 | 40 | 8 | 300 |
| 회장루 조성 개구에서 얻은 장액 | 130 | 15~20 | 120 | 25~30 | 8 | 300 |
| 설사 변 | 50 | 35 | 40 | 50 | 알카리성 | |
| 땀 | 50 | 5 | 55 | 0 | – | – |
| 혈액 | 140 | 4~5 | 100 | 25 | 7.4 | 285~295 |
| 소변 | 0~100 | 20~100 | 70~200 | 0 | 4.5~8.5 | 50~1,400 |
표 5-4, 표5-5 에서 볼 수 있는 것처럼 우리 몸의 각 기관에 있는 체액의 수분의 양, 전해질의 양, 산성도와 삼투압은 각각 다르다.
- 특히 체액의 성분 중
-
-
칼륨 이온(K⁺),
-
수소 이온(H⁺),
-
클로라이드(염화물) 이온(Cl⁻),
-
나트륨 이온(Na⁺),
-
중탄산기 이온(HCO3⁻) 등의 전해질 성분과 양은 신체의 각 기관의 체액의 종류에 따라 다른 것이 정상이다.
-
- 누구든지 설사를 할 때나,
-
땀을 비정상적으로 많이 흘릴 때,
-
그 외 다른 이유로 어떤 종류의 전해질이 비정상적으로 신체 내 외로 상실될 때
-
탈수의 정도와 종류에 따라 곧 대처해야한다.
-
- 이런저런 이유로 설사를 하게 되어 탈수가 됐을 경우, 전해질이 거의 들어있지 않는 맹물이나 보리차물 또 불균형 전해질 수액으로 설사나 구토로 생긴 탈수를 치료해서는 안 된다.
- 탈수의 정도, 상태, 종류, 전해질의 혈중 농도와 수분상실 정도, 탈수를 일으킨 원인 등에 따라 탈수의 증상 징후가 다르다.
- 각각의 요인에 따라 탈수증을 분류하는 법을 다음 표5-6에 소개한다.
| 탈수 정도에 따라 탈수 분류 |
- 총 체중의 5% 이하 신체 내 총 수분을 잃었을 때 탈수를 ‘경증(輕症) 탈수’ 또는 ‘경도 탈수’,
- 총 체중의 5~10% 신체 내 총 수분을 잃었을 때 탈수를 ‘중등도(中等度) 탈수’,
- 총 체중의 10%나 그 이상 신체 내 총 수분을 잃었을 때 탈수를 ‘중증도(重症度) 탈수’라 한다.
표 5-5. 영유아의 탈수의 정도 평가와 증상
| 탈수의 정도 | |||
| 관찰 또는 검진 내용 | 경도 탈수증(5%) | 중등도 탈수증(10%) | 중증 탈수증(15%) |
| 일반적 건강상태 | 갈증, 불안, 흥분 | 갈증, 불안, 과민반응 | 위축, 기면, 혼수, 빠르고 깊게 호흡 |
| 맥박 | 정상이고 | 빠르게 | 더 빠르게 |
| 맥박 상태 | 정상이고 | 약하고 | 약하고 촉지되기 어렵고 |
| 대천문을 만져보면 | 정상이고 | 움푹 들어가고 | 상당히 더 움푹 들어가고 |
| 눈 | 정상이고 | 움푹 들어가고 | 더 움푹 들어가고 |
| 울 때 눈물 | 눈물이 나고 | 눈물이 나지 않고 | 눈물이 나지 않고 |
| 점막과 입술 상태 | 약간 마르고 | 마르고 | 더 마르고 |
| 피부 긴장도 | 정상이고 | 감소되고 | 더 감소되고 텐트된다. |
| 피부를 만지면 | 정상이고 | 건조하고 | 친친한 감이 있다. |
| 소변 | 양이 정상일 수 있다. | 양이 감소될 수 있고 농도가 증가될 수 잇다 | 소변이 나오지 안해 몇 시간 동안 볼 수 없다 |
| 모세 혈관이 채워지는 시간 | 정상 | 2초 이내 | 3초 이상 걸린다. |
| 체중 감소 | 4~5% | 6~9% | 10% 이상 |
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition]다.
|
나트륨 이온(Na⁺)의 혈중 농도에 따른 탈수 분류 |
- 탈수가 되었을 때
-
-
혈 중 나트륨 이온(Na⁺)농도가 정상이면 ‘등장성 탈수증’,
-
정상 농도 보다 더 높으면 ‘고장성 탈수증’,
-
정상 농도 보다 더 낮으면 ‘저장성 탈수증’이라 한다.
-
- 어떤 병이나 다른 이유로 모유를 1~2회 먹지 못했거나, 인공영양, 이유식 또는 보통 음식물을 한두 번 못 먹었을 때는 경도 탈수가 생길 수 있다.
- 경도 탈수가 될 때는 기운이 없고, 소변 양이 줄고, 소변보는 간격이 보통 때보다 길고, 소변보는 횟수도 비정상적으로 줄어들고 갈증이 난다.
- 총 체중의 5~10%에 해당하는 체내 수분을 잃어 탈수가 되었을 때는 피부가 창백하고 건조해지고 피부에 윤기가 없어진다. 두 눈이 움푹 꺼져 들어가고, 눈․코․입의 점막에 물기가 거의 없어진다.
- 울어도 눈물이 거의 나지 않을 수 있다.
- 대천문(숨구멍)이 완전히 막히지 않은 영유아가 중등도 탈수되었을 때 대천문을 손으로 만져보면 대천문이 움푹 꺼져 들어갈 수 있다.
- 심장 박동이나 맥박도 평소보다 더 빠르거나 더 느려질 수 있다.
- 혈압이 비정상적으로 더 낮아질 수 있다.
- 소변은 평소 보다 상당히 적게 누고, 횟수도 더 줄어들고, 간격도 더 길어진다.
- 탈수가 계속되면 소변이 신장에서 전혀 분비되지 않기 때문에 소변을 조금도 보지 않는다.
- 영유아가 계속 토하거나, 설사하거나, 구토와 설사를 동시에 하면서 열이 나면 짧은 시간 내 중증 탈수로 이어질 수 있다.
- 체중의 15%에 해당하는 체내 수분을 잃어 중증 탈수가 되면 쇼크에 빠질 수 있고 사망 직전에 이르거나 사망할 수 있다.
표 5-6. 등장성 탈수증, 저장성 탈수증, 고장성 탈수증의 증상 징후
| 탈수증의 종류
검진 내용 및 전해질 |
등장성 탈수증 | 저장성 탈수증 | 고장성 탈수증 |
| 혈청 나트륨(Na+)의 농도 (mEq/L) | 130~150 | 130 이하 | 150 이상 |
| 피부색 | 회색(Gray) | 회색(Gray) | 회색(Gray) |
| 피부의 온도 | 차다 | 차다 | 차다 |
| 피부의 팽만감(Turgor) | 비정상 | 상당히 비정상 | 조금 비정상 |
| 촉감 | 건성 | 촉촉한 감 | 밀가루 반죽을 만지는 것과 같은 촉감 |
| 점막 | 마름 | 마름 | 바싹 마름 |
| 눈이 움푹 꺼진다, 안 꺼진다 | 꺼진다. | 꺼진다. | 꺼진다. |
| 움푹 꺼진 숨구멍을 만져 볼 수 있다. 또는 없다 | 있다 | 있다 | 있다 |
| 정신 상태 (++++은 가장 정상적임, +은 아주 좋지 않음) | ++/++++ | ++/++++ | +/++++ |
| 혈압의 감소 (++++은 가장 정상적임, +은 아주 낮음) | ++ | +++ | + |
[참고 Infectious Diseases In Children p.18, Vol 17 #5 May 2004 & CDC,
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition,
Emergency Pediatrics 5th, Roger M Barkin, Peter Rosen p70]
| 탈수증의 진단 |
- 탈수로 생긴 증상 징후를 탈수증이라 한다.
- 탈수는 어떤 병에서 생기는 증상이다.
- 따라서 가능한 한 탈수를 일으킨 원인을 신속히 찾아내야 한다.
- 병원에서는 과거·현재 가족의 병력, 증상 징후와 진찰소견 등을 종합하고 필요에 따라 대소변 검사, 피검사 등을 해서 탈수증을 일으킨 원인을 찾아 진단한다.
- 탈수가 되기 직전 체중 치와 탈수가 된 이후 체중 치가 얼마인지 알면 그 두 체중 치의 차이로 체중의 몇 %가 감소했는지 알아보고 수분을 얼마나 잃었는지 알고 탈수의 정도를 쉽게 알 수 있다.
- 그렇지만 대부분의 경우, 탈수되기 바로 전 체중을 확실히 알 수 없다.
- 따라서 앞에 있는 도표(표5-6, 5-7)에 있는 증상 및, 징후를 참작해 임상적으로 탈수의 정도를 알아내는 경우가 더 많다.
- 혈중 전해질 농도, 소변검사, 피검사, 체중 증감 등으로 탈수증의 정도를 종합해서 알아낼 수 있다.
| 탈수증의 치료 |

사진 4-158. 페디아라이트(Pedialyte, Ross회사) 등 경구용 포도당 전해질 용액으로 경미한 설사와 탈수를 치료하고 예방할 수 있다.
이런 약물은 약국에서 의사의 처방 없이 사서 의사의 지시에 따라 또는 부모의 자녀양육, 가정간호 지식에 따라 부모들이 또는 비 의료인들이 쓸 수 있는 포도당 전해질 수액이다.
이런 전해질 약물을 부모들이 쉽게 사서 치료할 수 있으므로 죽을 수 있는 숱한 생명을 구할 수 있으니 얼마나 다행인지 모른다.
그러나 어떤 나라에서는 의사의 처방 없이 살 수 없다.
Copyright ⓒ 2011 John Sangwon Lee, MD/, FAAP
그림 4-34. 혈관주사용 포도당 전해질용액으로 설사와 탈수를 재수화 치료를 하고 탈수 현상유지 수화 치료를 할 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- 탈수증의 정도와 탈수를 일으킨 질병에 따라 탈수 치료법도 다르다.
- 일반적으로 나이가 어리면 어릴수록, 구토 및, 또는 설사를 하거나 열이 많이 날수록 쉽게 탈수되고 탈수증이 심하게 생긴다.
- 탈수의 증상과 정도 등에 따라 의료 구급대나 병원 응급실, 단골 소아청소년과 의사에게 전화해서 그들의 지시에 따라 가정 탈수치료를 시작한다.
- 중등(中等)도 탈수 내지 중증(重症) 탈수가 되었다고 의심되면 구급차나 그 외 다른 교통수단을 이용해 최대한 빨리 병원 응급실로 데리고 가야 한다.
- 병원에서는 가능한 한 의사가 지시한 경구용 포도당 전액질 용액 이외 아무 음식물도 먹이지 말아야 한다. p000 설사 치료에 쓰는 전해질 용액의 종류와 성분표, 설사 참조)
표 5-8.설사와 탈수 치료에 쓸 수 있는 경구용 포도당 전해질 재수화(Rehydration) 용액, 경구용 포도당 전해질 현상 유지(Maintenance) 용액, 전 유동 음식물의 전해질 농도, 포도당 농도, 삼투압의 비교표
| 설사와 탈수 치료를 할 때 쓸 수 있는 경구용 재수화 용액, 경구용 현상유지 수화 치료 용액, 전유동 음식물의 전해질과 포도당의 농도, 삼투압 등의 비교표 | ||||||
| 경구용 포도당과 전해질 재수화 용액 | Na+ nM/L | K+ nM/L | Cl- nM/L | HCO3- mEq/L | 포도당/L (%) | mosM |
| 1. 설사와 탈수를 응급으로 치료할 때 주로 쓰는 경구용 재수화 용액 | ||||||
| WHO에서 권장하는 경구용 재수화 용액 (Oral Rehydration Solution) | 90 | 20 | 80 | 30 | 111(2%) | 310 |
| 리하이드라라이트 재수화 용액 (Rehydralyte solution) (Ross 회사) | 75 | 20 | 65 | 30 | 139 (2.5%) | 305 |
| 2. 더 이상 탈수되지 않게 치료할 때 주로 쓰는 경구용 현상유지 수화 용액 | ||||||
| 페디아라이트 용액 (Pedialyte solution) (Ross 회사) | 45 | 20 | 35 | 30 | 139 (2.5%) | 250 |
| 인파라이트 용액 (Infalyte solution) (Pennwalt 회사) | 50 | 20 | 40 | 30 | 111 (2%) | 270 |
| 라이스라이트 용액(Ricelyte solution) (Mead Johnson 회사) | 50 | 25 | 45 | 0 | 3% | 0 |
| 3. 설사와 탈수를 치료할 때 재수화 용액으로 써서도 안 되고 의사의 지시에 따라 현상유지 수화 용액으로 쓸 수 있는 전 유동식 또는 반 유동식 | ||||||
| 가타라데 (Gatarade) | 23 | 3 | 17 | 3 | 255 | 330 |
| 콜라 (Cola) | 2 | 0.1 | 2 | 13 | 730 | 750 |
| 쿨 에이드 (Kool-Aid) | 3 | 0.1 | 0 | 0 | 105 | 465 |
| 사과 주스 (Apple juice) | 3 | 28 | 30 | 0 | 690 | 725 |
| 하이 시 (Hi-C) | 2 | 5 | 0 | 0 | 800 | 816 |
| 팝씨클 (Popsicle) | 5 | 0.5 | 0 | 0 | 710 | 719 |
| 닭고기 국물 (Chicken broth) | 251 | 8 | 250 | 0 | 0 | 501 |
| 맹물 | 0 | 0 | 0 | 0 | 0 | – |
주: 적절한 현상 유지 수화 치료용액은 5-10% Dextrose와 0.2% NaCl + 20 mEq/L KCl 또는 K acetate이다.
참고: 경구용 포도당 전해질 현상유지 용액과 재수화 용액은 비 의료인들이 의사의 처방 없이 사서 쓸 수 있게 법으로 정하면 좋을 것이라고 생각한다.
※ 적절한 현상유지수화 장관 외 수액 치료용액은 포도당 용액 5-10%와 0.2% NaCl(소금물) + 20 mEq/L(리터당 밀리그램당량) KCl(염화칼륨) 또는 K acetate이다.
표 각 중상이나 병에 따른 100칼로리 당 필요한 1일 수분과 Na⁺, K⁺ 전해질 이온의 필요량
Average water and electrolyte requirements per 100 calories per 24 hours
| 병명, 증상, 임상적 상태 | H₂O(물)ml | Na⁺ mEq | K⁺ mEq |
| 평균 장관 외 수액 필요량 | 100-120 | 2-4 | 2-3 |
| 무요증 | 45 | 0 | 0 |
| 급성 중추신경 감염병과 염증 | 80-90 | 2-4 | 2-3 |
| 요붕증 | 400까지 | 그때그때에 따라 변함 | 그때그때에 따라 변함 |
| 과도 호흡 | 120-210 | 2-4 | 2-3 |
| 열, 스트레스 | 120-240 | 그때그때에 따라 변함 | 그때그때에 따라 변함 |
| 고습 환경 | 80-100 | 2-4 | 2-3 |
적절한 현상유지수화 장관 외 수액 치료용액은 포도당 용액 5-10%와 0.2% NaCl(소금물) + 20 mEq/L(리터당 밀리그램당량) KCl(염화칼륨) 또는 K acetate이다.
[참고 The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p302-311, Nelson text book, 14 edition p.198-199,Quick Reference to Pediatric Emergencies, Delmer J. Pascoe, M.D., p.191,
Emergency Pediatrics, A guide to ambulatory care, 5th edi. Roger M. Barkin, Peter Rosen, p. 69-77, 67-82,
Emergency care and transportation of the sick and injured, 3rd edition, American Academy of orthopedic surgeons. p.69, 240, 277]
|
다음은 “아이가 열이 나고 토하고 설사를 해요, ‘위장염과 탈수‘”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q.&A. 아이가 열이 나고 토하고 설사를 해요.
Q.
- 저희 아기는 9개월인데요. 이틀 전부터 열이 39도가 넘고 설사를 하더니 좀 울다보면 토하더군요. 병원에 갔더니 감기인 것 같다는데 먹는 해열제를 주면 토해서 서스펜 좌약을 넣으면 12시간 괜찮다가, 또 열이 오르고, 먹는 약을 주면 토해 버리고, 비위가 대단히 약해져 있습니다. 우유도 50~70 밖에 먹질 못하고 힘이 없어요. 오늘도 약을 먹였더니 토했는데 보니까 가래 같은 게 섞어있던데 약을 먹여도 안 되니 감기가 아닌 다른 게 아닐까요.
- 옛날에 제 둘째 녀석이 아플 때 하도 안 나아서 다른 병원에 갔더니 열을 내야 낫는다고 해서 발열 주사를 줘서 맞고 열을 내고 나았던 적이 있는데 혹시 얘도 그런 게 아닐까 하고요. 감기인데 콧물도 없고 기침도 어쩌다 한 번씩만 하고 정말 맞을까요? 요즘 감기가 이런가요? 혹시 홍역이 아닌지요. 너무 걱정이 됩니다. 꼭 답장 부탁드릴게요. 수고하세요.
A.
- 언니님
- 안녕하십니까. 질문해 주셔서 감사합니다. 자녀의 나이와 성별, 과거 현재 가족의 병력, 증상 증후와 진찰소견, 적절한 임상검사 등의 결과를 종합해서 진단 치료하는 것이 이상적이지만 주신 정보를 참작해서 답변을 드립니다.
- 영아에게 고열이 나고 토하고 설사하는 증상 징후가 있으면 많이 아픈 것입니다.
- 그런 증상 징후를 가진 영아는 응급으로 치료해야 합니다.
- 그런 증상들을 나타낼 수 있는 원인이 무엇인지 알아내는 것도 중요합니다.
- 그런 증상들이 계속되면 짧은 시간 이내 심하게 탈수가 될 수 있고, 전해질 불균형이 생겨 때로는 생명에 상당히 위험할 수 있습니다.
- 탈수는 경도탈수, 중등도 탈수, 중증 탈수로 분류됩니다.
- 아기의 경우 적어도 중등도 탈수가 됐을 것입니다.
- 그런 증상 징후가 있으면서 중등도 탈수가 됐으면 포도당 전해질용액 정맥주사 등으로 우선 재수화 치료를 응급으로 해야 합니다.
- 그와 동시에 무슨 원인으로 그런 증상 징후가 생겼나 알아보고 그 원인에 따른 치료해야 됩니다.
- 토하고 설사하고 열나는 원인이 무엇인지 저도 확실히 모르겠습니다.
- 그러나 바이러스성 위장염, 박테리아성 위장염, 식중독 등으로 그런 증상 징후가 나타날 수 있습니다.
- 어떤 원인으로 인해서 위장관 내 음식물이 소화될 수 없기 때문에 토하고 설사를 하는 것입니다.
- 다시 설명하면, 위장염이 있을 때는 상·하부 위장관 중 상부 위장관 속에 있는 먹은 위 내 음식물이나 위장관 벽 점막층에서 분비된 위장 액을 토해 식도, 입을 통해 체외로 내보내고, 상하부 위장관 중 하부 위장관 속에 있는 소장관, 대장관 내 먹은 음식물이나 위장관 벽 점막층에서 나오는 장액, 취장액, 담즙 등이 섞인 “위장관 내 혼합물”은 소대장관→ 항문을 통해 설사 변으로 체외로 내보내게 됩니다.
- 이런 때는 위장관에 생긴 이상이 다 나을 때까지 모유, 인공영양물 등 모든 종류의 음식물을 경구로 먹이지 말고, 몇 시간 내지 드물게는 하루 이틀 동안 위장관 기능을 쉬게 해야 합니다.
- 특히 열나고 구토 설사를 할 때는 더욱 그렀습니다.
- 그 대신 포도당 전해질용액 정맥주사 등으로 탈수와 전해질 불균형을 재수화 치료하고 현상유지 수화 치료를 해야 합니다.
- 열이 나고 구토에서 설사까지 하는 영아에게 모유를 비롯해서 아무것도 먹이지 않으면 탈수가 쉽게 될 것입니다.
- 따라서 위에서 말씀드린 대로 포도당 전해질용액 정맥주사로 재수화 탈수 치료를 하고, 정상적으로 그날그날 필요로 한 수분과 전해질량을 공급해주는 현상유지 수화치료를 해야 합니다.
- 그러기 위해서는 의사의 진단치료를 급히 받아야 합니다.
- 우유나 우유로 만든 음식물, 유당이든, 인공영양을 섭취하는 것은 이 경우 금기입니다
- 타이레놀 등 해열제로 열을 해열시키는 것은 아주 쉬운 해열 치료법입니다.
- 그러나 열나게 하는 원인을 안 후나, 적어도 추정한 이후 의사의 지시에 따라서 타이레놀 등 해열제로 해열시켜야 합니다.
- 옛날에는 발열시켜 치료하는 법을 썼지만 요즘 의학계에서는 그런 치료 법을 전혀 쓰지 않습니다.
- 다시 한 번 말씀드리지만 열이 나는 원인을 아시고 또는 적어도 추정하고 그 원인에 따라 치료해야 합니다. 질문이 더 있으면 또 방문하세요. 감사합니다. 이상원 드림
Acute dehydration in breastfeeding infant 젖 먹는 아기에게 생긴 급성 탈수증
1. Body moisture, electrolyte balance and dehydration
- The phenomenon in which the total amount of water in the body becomes less than normal is called ‘dehydration.
- ’ The symptom of dehydration is ‘dehydration’,
- Sudden dehydration is ‘acute dehydration’,
- Chronic dehydration is called chronic dehydration.
- Dehydration can occur in newborns, infants, school-age children, adolescents, and anyone of any age.
- However, dehydration can occur more easily and more severely, especially in infants and toddlers.
- Fortunately, vomiting and or diarrhea are less common in breastfeeding infants.
- 80% of the total body weight of premature newborns, 65% of the total body weight of a 1-year-old infant, 60% of an adult’s total body weight is water.
- The daily water ingested orally and electrolytes such as K⁺, H⁺, Cl⁻, Na⁺, and HCO3⁻ pass through the mucous membrane of the gastrointestinal tract and are absorbed into the blood.
- Water and electrolytes consumed more than necessary are excreted from the body through urine, feces, and sweat.
- The total amount of water in the body and the total amount of electrolytes are kept constant, and electrolytes are balanced.
- When the body contains more water and electrolytes than necessary, more water and electrolytes than necessary are discharged from the body through the skin, respiratory tract, urinary tract, and gastrointestinal tract.
- If an infant is unable to eat or drink any of the breast milk, artificial nutrition, baby food, meals at the table, or due to some disease, water and electrolytes are not adequately replenished, the body’s water and electrolytes are not discharged if possible.
- Sodium ions (Na+), potassium ions (K+), chloride ions (Cl-), bicarbonate ions (HCO3-), and other electrolytes and water balance in the body are achieved.
- Dehydration and electrolyte imbalance can occur when you lose more fluids and electrolytes out of the body than the amount of fluid you ingest or the amount of electrolytes for some disease, starvation, or other reasons.
- When dehydrated, not only a part of the body’s total water is lost, but electrolytes such as sodium ions, potassium ions, and chloride ions are also lost. At the same time, the blood can be acidified or alkalized.
- In particular, infants and toddlers can become severely dehydrated when they have diarrhea or vomiting due to viral gastroenteritis or bacterial gastroenteritis.
- At this time, if you do not eat any kind of food such as breast milk, artificial nutrition, baby food, etc., dehydration and loss of electrolytes may occur, resulting in dehydration and electrolyte imbalance. Indigestible food, breast milk, or artificial nutrition, partially digested food, water secreted into the gastrointestinal tract through the mucous membrane of the gastrointestinal tract from the blood vessels, electrolytes, gastrointestinal fluid secreted from the mucous membrane of the gastrointestinal tract, pancreatic juice, bile, etc.
- It becomes a mixture in the gastrointestinal tract.
- When suffering from gastroenteritis, the mixture in the gastrointestinal tract passes through the mucous membrane of the gastrointestinal tract and cannot be absorbed normally into the blood, and is excreted in the small intestine → colon → anus. In other words, the mixture in the gastrointestinal tract becomes diarrhea.
- Even when vomiting, undigested food and gastric juice in the upper gastrointestinal tract vomit and come out of the mouth.
- This phenomenon is called vomiting.
- The contents of the stomach are vomit. If a part of the lower intestine duct below the duodenal duct is blocked, you can vomit food and gastric juice you eat, and you can vomit a “mixture in the gastrointestinal tract” that is a mixture of pancreatic juice, bile juice, and intestinal fluid secreted from the mucous membrane of the intestinal wall.
- At this time, you can have filtration diarrhea’. In other words, when diarrhea and vomiting, most of diarrhea or vomiting water is a mixture of food, breast milk, artificial nutrition, baby food, etc. that have passed through the mucous membrane of the gastrointestinal tract from the blood vessels. It is “a mixture in the gastrointestinal tract”.
- When vomiting and or diarrhea, it is common for dehydration to occur as the water and electrolytes in the body’s blood decrease below normal and the total amount of water and electrolytes in the body decreases.
- For reference, the physiology following diarrhea and vomiting is described. It will be very helpful in treating diarrhea and vomiting (parents should also be at least the half-doctors-Encyclopedia of Pediatrics and Family Nursing-Volume 9 Children and Adolescents Digestive Diseases-Rotavirus gastroenteritis, gastroenteritis due to rotavirus infection).
Photo 4-157. Diarrhea stool. Diarrhea is when undigested food and the mucous membrane of the gastrointestinal tract are mixed with water and intestinal fluid that has not been absorbed into thin stools. The intestinal fluid contains electrolytes. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 4-33. When the mucous membrane of the gastrointestinal tract is damaged or swollen due to gastroenteritis, the movement of electrolytes and water during diarrhea, and the composition of diarrhea.
Electrolytes such as potassium ions (K+), hydrogen ions (H+), chloride ions (Cl-), sodium ions (Na+), and bicarbonate ions (HCO3-) are mixed with intestinal fluids and undigested foods, causing diarrhea to excrete abnormally in feces.
. This stool is called diarrhea. Sudden diarrhea can lead to dehydration, loss of electrolytes, electrolyte imbalance, and changes in blood acidity (pH). Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
2. Causes of dehydration
- Newborns, infants and toddlers who are fed breast milk or artificial nutrition, or infants and toddlers who eat meals at the table, and school-age children without any disease, without eating one or two meals, and starving can lead to mild dehydration and more dehydration.
- Even if you don’t have diarrhea or vomiting from any disease, starving for a meal or two can lead to dehydration.
- When you consume too much soy sauce or salt,
- When you eat a lot of food very salty,
- When vomiting and diarrhea for any cause,
- When treating diarrhea with boiled skim milk Salt poisoning and/or hypertonic dehydration may occur.
- Diarrhea and vomiting caused by gastroenteritis and dehydration can be treated with a homemade oral electrolyte solution.
- However, when making an oral electrolyte solution for the treatment of diarrhea and/or diarrhea at home, the amount of salt or soda that is wrongly added or less than the recommended amount is used to make an oral electrolyte solution for home use, or for home oral use that is made incorrectly.
- Excessive intake of electrolyte solutions can lead to salt poisoning or hypertonic dehydration.
- Acute dehydration can also result from severe diarrhea and vomiting due to untreated type 1 diabetes, poorly treated type 1 diabetes, viral gastroenteritis or bacterial gastroenteritis.
- In rare cases, vomiting from pyloric stenosis can lead to dehydration and electrolyte imbalance.
- In addition, when suffering from severe burns, bleeding, or other diseases, eating small amounts of food and drinking small amounts of water can lead to dehydration.
- In particular, when newborns or infants cannot eat or drink due to gastroenteritis, vomiting, diarrhea, or fever, they can become severely dehydrated within a short period of time.
3. Signs, symptoms of dehydration
Table 5-4. Electrolyte component (pH) and osmotic pressure of body fluids in each organ of the body 표 5-4. 신체 각 기관의 체액의 전해질 성분(pH)과 삼투압
| 130 | 5 | 100 | 40 | 8 | 300 | |
| Serous fluid obtained from the opening of the ileum composition | 130 | 15~20 | 120 | 25~30 | 8 | 300 |
| Diarrhea stool | 50 | 35 | 40 | 50 | 알카리성 | |
| Sweat | 50 | 5 | 55 | 0 | – | – |
| Blood | 140 | 4~5 | 100 | 25 | 7.4 | 285~295 |
| Urine | 0~100 | 20~100 | 70~200 | 0 | 4.5~8.5 | 50~1,400 |
As can be seen in Tables 5-4 and 5-5, the amount of water, electrolytes, acidity and osmotic pressure in each organ of our body are different.
Especially among the components of body fluids
1. Potassium ion (K⁺),
2. Hydrogen ion (H⁺),
3.Chloride (chloride) ion (Cl⁻),
4. Sodium ion (Na⁺),
5. It is normal that the electrolyte components and amounts such as
bicarbonate ions (HCO3⁻) differ depending on the type of fluid in each
organ of the body.
- Whenever anyone has diarrhea, When you sweat abnormally much, When some kind of electrolyte is abnormally lost in and out of the body for any other reason.
- Depending on the degree and type of dehydration, you will have to deal with it soon.
- If you are dehydrated due to diarrhea for one or the other reasons, you should not treat dehydration caused by diarrhea or vomiting with plain water, barley tea, or unbalanced electrolyte fluids that contain little electrolytes.
- Symptoms of dehydration differ depending on the degree, condition, and type of dehydration, the level of electrolytes in the blood and the degree of water loss, and the cause of the dehydration.
- Table 5-6 introduces how to classify dehydration according to each factor.
Classification of dehydration according to the degree of dehydration
- When you lose 5% or less of your total body weight, dehydration is called ‘mild dehydration ,
- When you lose 5-10% of the total body weight, dehydration is called ‘moderate dehydration’,
- Dehydration is called ‘severe dehydration when you lose 10% or more of your total body weight.
Table 5-5. Evaluation and symptoms of dehydration in infants and toddlers 표 5-5. 영유아의 탈수의 정도 평가와 증상
| Degree of dehydration | |||
| Observation or examination details | Mild dehydration(5%) | Moderate dehydration(10%) | Severe dehydration(15%) |
| General health conditions | Thirst, anxiety, excitement, thirst, | thirst, anxiety, hypersensitivity | withdraw, lethargy, coma, breathing quickly and deeply |
| Pulse normal | normal | fast | faster |
| Pulse status | normal | weak | weak, difficult to palpate |
| Anterior fontanel palpation | normal | sunken | more sunken |
| eyes | normal | sunken | more sunken |
| tearing when crying | tear | no tear in crying | no tear in crying |
| mucous membrane and lips | slightly dry | dry | drier |
| Skin tension | normal | decreased | more decreased and tenting |
| When touching skin | normal | dry | drier |
| urine | The amount of urine may be normal. | Volume may be reduced and concentration may be increased. | Urine does not come out and cannot be seen for several hours |
| time of filling the capillary vessel | normal | within 2 seconds | It takes 3 seconds or more |
| weight loss | 4~5% | 6~9% | 10% or more |
Classification of dehydration according to the blood concentration of sodium ions (Na⁺)
• When you become dehydrated
o If the sodium ion (Na⁺) concentration in the blood is normal, ‘isotonic dehydration,
o If it is higher than the normal concentration, ‘hypertonic dehydration,
o If the concentration is lower than the normal concentration, it is called ‘hypotonic dehydration.
• Mild dehydration may occur if one or two times of breast milk has not been eaten for some disease or other reason, or if one or two times of artificial nutrition, baby food, or regular foods have not been eaten.
• When mild dehydration occurs, there is no energy, the amount of urine decreases, the interval between urination is longer than usual, the number of urinations is abnormally reduced, and thirst is generated.
• When the body loses moisture equivalent to 5-10% of the total body weight and becomes dehydrated, the skin becomes pale and dry, and the skin loses its shine. Both eyes are pitted, and the moisture in the mucous membranes of the eyes, nose, and mouth almost disappear.
• Crying with little tears.
• Your heart rate or pulse may also be faster or slower than usual.
• Blood pressure may be abnormally lower.
• Urinate significantly less than usual, fewer times, and longer intervals.
• If dehydration continues, do not urinate at all because no urine is secreted by the kidneys.
• Infants and toddlers who continue to vomit, have diarrhea, or have a fever while vomiting and diarrhea at the same time can lead to severe dehydration within a short period of time.
• Severe dehydration due to the loss of water in the body equivalent to 15% of the body weight can lead to shock, shortly before death or death.
Table 5-6. Symptoms, signs of isotonic dehydration, hypotonic dehydration, hypertonic dehydration 표 5-6. 등장성 탈수증, 저장성 탈수증, 고장성 탈수증의 증상 징후
| Types of dehydration,
Examination details and electrolyte |
isotonic dehydration | hypotonic dehydration | hypertonic dehydration |
| Serum sodium (Na+) concentration(mEq/L) | 130~150 | 130 이하 | 150 이상 |
| Skin Color | Gray | Gray | Gray |
| Skin temperature | cold | cold | cold |
| Skin Turgor | abnormal | very abnormal | somewhat abnormal |
| Skin feeling | dry | somewhat wet feeling | like feeling to touch the dough |
| mucous membrane | dry | dry | very dry |
| anterior fontanel | sunken | sunken | sunken |
| sunken anterior fontanel | able to feel | able to feel | able to feel |
| Mental state-(++++ is the most normal, + is very bad | ++/++++ | ++/++++ | +/++++ |
| Decreased blood pressure (++++ is the most normal, + is very low) | ++ | +++ | + |
Diagnosis of dehydration
• Dehydration is a symptom of certain diseases.
• Therefore, it is important to find out the cause of dehydration as quickly as possible.
• At the hospital, the family’s medical history, symptoms, and examination findings are synthesized, and if necessary, feces and blood tests are performed to find and diagnose the cause of dehydration.
• If you know your body weight just before dehydration and how much your body weight has been after dehydration, you can find out what percentage of your body weight is lost due to the difference between the two body weights, know how much water you have lost, and easily determine the degree of dehydration.
• However, in most cases, you cannot be sure of your baby’s weight right before your baby becomes dehydrated.
• Therefore, it is more common to determine the degree of dehydration clinically by taking into account the symptoms and signs in the preceding chart (Tables 5-6 and 5-7).
• You can find out the degree of dehydration by synthesizing the level of dehydration through blood electrolyte concentration, urine test, blood test, and weight gain.
Treatment of dehydration
Photo 4-158. It can treat and prevent mild diarrhea and dehydration with oral glucose electrolyte solutions such as Pedialyte (Ross company).
These drugs are glucose electrolyte fluids that can be bought at a pharmacy without a doctor’s prescription and used by parents or non-medical practitioners as directed by a doctor or as a parent’s knowledge of child-rearing and home care.
Parents can easily buy and treat these electrolytes, so we don’t know how fortunate they can save countless lives. However, in some countries, you cannot live without a doctor’s prescription. Copyright ⓒ 2011 John Sangwon Lee, MD/, FAAP
Figure 4-34. It is possible to rehydrate diarrhea and dehydration with a glucose electrolyte solution for intravascular injection and to maintain dehydration and hydration. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• Treatment for dehydration depends on the degree of dehydration and the disease that caused it.
• In general, the younger the person is, the more vomiting and/or diarrhea or fever they are, the more easily they become dehydrated and more dehydrated.
• Depending on the symptoms and severity of dehydration, call a medical paramedic, hospital emergency room, or a regular pediatrician and follow their instructions to begin home dehydration treatment.
• If you suspect you have moderate or severe dehydration, you should take an ambulance or other means of transportation to the hospital emergency room as soon as possible.
• Hospitals should avoid feeding any food other than the oral glucose full solution as directed by a doctor whenever possible. Type of electrolyte solution used to treat diarrhea and ingredient table, refer to diarrhea
Table 5-8. Comparison of oral glucose electrolyte rehydration solution, oral glucose electrolyte maintenance solution, electrolyte concentration of whole food, glucose concentration, and osmotic pressure that can be used to treat diarrhea and dehydration
표 5-8.설사와 탈수 치료에 쓸 수 있는 경구용 포도당 전해질 재수화(Rehydration) 용액, 경구용 포도당 전해질 현상 유지(Maintenance) 용액, 전 유동 음식물의 전해질 농도, 포도당 농도, 삼투압의 비교표
| 설사와 탈수 치료를 할 때 쓸 수 있는 경구용 재수화 용액, 경구용 현상유지 수화 치료 용액, 전유동 음식물의 전해질과 포도당의 농도, 삼투압 등의 비교표
Comparison table of electrolyte and glucose concentrations, osmotic pressure, etc. of oral rehydration solution for diarrhea and dehydration treatment, oral status maintenance hydration treatment solution |
||||||
| 경구용 포도당과 전해질 재수화 용액 Oral glucose and electrolyte rehydration solution | Na+ nM/L | K+ nM/L | Cl- nM/L | HCO3- mEq/L | 포도당/L (%) | mosM |
| 1. 설사와 탈수를 응급으로 치료할 때 주로 쓰는 경구용 재수화 용액
1. Oral rehydration solution mainly used for emergency treatment of diarrhea and dehydration |
||||||
| WHO에서 권장하는 경구용 재수화 용액 (Oral Rehydration Solution)
Oral Rehydration Solution recommended by WHO |
90 | 20 | 80 | 30 | 111(2%) | 310 |
| 리하이드라라이트 재수화 용액 (Rehydralyte solution) (Ross 회사) | 75 | 20 | 65 | 30 | 139 (2.5%) | 305 |
| 2. 더 이상 탈수되지 않게 치료할 때 주로 쓰는 경구용 현상유지 수화 용액
2. Oral status quo hydration solution mainly used to treat dehydration |
||||||
| 페디아라이트 용액 (Pedialyte solution) (Ross 회사)
Pedialyte solution (Ross company) |
45 | 20 | 35 | 30 | 139 (2.5%) | 250 |
| 인파라이트 용액 (Infalyte solution) (Pennwalt 회사)
Infalyte solution (Pennwalt company) |
50 | 20 | 40 | 30 | 111 (2%) | 270 |
| 라이스라이트 용액(Ricelyte solution) (Mead Johnson 회사)
Ricelyte solution (Mead Johnson company) |
50 | 25 | 45 | 0 | 3% | 0 |
| 3. 설사와 탈수를 치료할 때 재수화 용액으로 써서도 안 되고 의사의 지시에 따라 현상유지 수화 용액으로 쓸 수 있는 전 유동식 또는 반 유동식
3. A full or semi-fluid formula that should not be used as a rehydration solution for the treatment of diarrhea and dehydration and that can be used as a status quo hydration solution as directed by a physician |
||||||
| 가타라데 (Gatorade) | 23 | 3 | 17 | 3 | 255 | 330 |
| 콜라 (Cola) | 2 | 0.1 | 2 | 13 | 730 | 750 |
| 쿨 에이드 (Kool-Aid) | 3 | 0.1 | 0 | 0 | 105 | 465 |
| 사과 주스 (Apple juice) | 3 | 28 | 30 | 0 | 690 | 725 |
| 하이 시 (Hi-C) | 2 | 5 | 0 | 0 | 800 | 816 |
| 팝씨클 (Popsicle) | 5 | 0.5 | 0 | 0 | 710 | 719 |
| 닭고기 국물 (Chicken broth) | 251 | 8 | 250 | 0 | 0 | 501 |
| 맹물 fresh water | 0 | 0 | 0 | 0 | 0 | – |
A suitable maintenance-hydrating parenteral fluid treatment solution is a glucose solution of 5-10% and 0.2% NaCl (brine) + 20 mEq/L (milligram equivalents per liter) KCl (potassium chloride) or K acetate.
[See The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p302-311, Nelson text book, 14 edition p.198-199,Quick Reference to Pediatric Emergencies, Delmer J. Pascoe, M.D., p.191, Emergency Pediatrics, A guide to ambulatory care, 5th edi. Roger M. Barkin, Peter Rosen, p. 69-77, 67-82,
Emergency care and transportation of the sick and injured, 3rd edition, American Academy of orthopedic surgeons. p.69, 240, 277]
The following is an example of a Q&A on health counseling for children and adolescents on the Internet about “the child has a fever, vomiting, and diarrhea, ‘gastroenteritis and dehydration’”.
Q&A.
The child has a fever, vomits and has diarrhea.
Q.
• My baby is 9 months old. Two days ago, I had a fever of over 39 degrees and had diarrhea.
After crying a little, I vomited. When I went to the hospital, it seems like I have a cold, but if I give him an antipyretic drug, he vomits, and if I put a suspen suppository, it’s fine for 12 hours.
I can only eat 50-70 milk and I have no energy. I took medicine today, and I vomited, but it was mixed with phlegm.
• Once upon a time, when my second child was ill, he didn’t get better, so he went to another hospital and he said that he had to have a fever to get better. It’s a cold, but I don’t have a runny nose and cough only once in a while. Is it really okay? How is your cold these days? Maybe it’s measles? I’m so worried. Please be sure to reply. work hard.
A.
• Sister
• Hello. Thanks for asking. It is ideal to diagnose and treat the child’s age and gender, past and present family history, symptom symptoms, examination findings, and appropriate clinical examination results, but we will respond taking into account the information provided.
• If your baby has a high fever, vomiting, and signs of diarrhea, they are very ill.
• Infants with any of these symptoms should be treated urgently.
• It is also important to find out what could be causing these symptoms.
• If these symptoms persist, you can become severely dehydrated within a short period of time, resulting in an electrolyte imbalance, which can sometimes be quite life-threatening.
• Dehydration is classified as mild dehydration, moderate dehydration, and severe dehydration.
• Your baby will be at least moderately dehydrated.
• If you have such symptoms and become moderately dehydrated, you should first receive treatment for rehydration, such as intravenous glucose electrolyte solution, as an emergency.
• At the same time, you need to find out what caused the symptoms and treat them accordingly.
• I’m not sure what causes vomiting, diarrhea and fever.
• However, viral gastroenteritis, bacterial gastroenteritis, or food poisoning can cause such symptoms.
• Vomiting and diarrhea because food in the gastrointestinal tract cannot be digested for some reason.
• In other words, when gastroenteritis is present, the food in the stomach in the upper gastrointestinal tract of the upper and lower gastrointestinal tracts or gastrointestinal fluid secreted from the mucosal layer of the gastrointestinal tract is discharged out of the body through the esophagus and mouth, and the small intestine is located in the lower gastrointestinal tract among the upper and lower gastrointestinal tracts.
The “mixture in the gastrointestinal tract,” which is mixed with food eaten in the large intestine or intestinal fluid from the mucosal layer of the gastrointestinal tract wall, is expelled from the body as diarrheal feces through the small intestine → anus.
• In this case, do not orally feed any kind of food, such as breast milk or artificial nutrients, until the gastrointestinal tract is completely healed, and the gastrointestinal function should rest for a few hours or, in rare cases, a day or two.
• Especially with fever and vomiting and diarrhea. • Instead, rehydration treatment for dehydration and electrolyte imbalance, such as intravenous injection of glucose electrolyte solution, and maintenance hydration treatment should be performed.
• Infants who have a fever and are vomiting to diarrhea will become dehydrated if they are not fed anything, including breast milk.
• Therefore, as mentioned above, rehydration and dehydration treatment by intravenous injection of glucose electrolyte solution should be performed, and maintenance hydration treatment that normally supplies the amount of water and electrolytes needed each day.
• To do so, you must urgently seek medical attention.
• Contraindicated in this case to consume milk, food made from milk, lactose, or artificial nutrition.
• Relieving fever with an antipyretic drug such as Tylenol is a very easy antipyretic treatment.
• However, after knowing the cause of the fever, or at least after estimating it, you should treat it with an antipyretic such as Tylenol according to the doctor’s instructions.
• In the past, there was a method of treating fever with fever, but these days the medical world does not use such a treatment method at all.
• Again, the cause of the fever must be known or at least estimated and treated according to the cause. Please visit again if you have more questions. thank you. Lee Sang-won
출처 및 참조 문헌
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding by Ruth Lawrence and Robert Lawrence
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
- The Harriet Lane Handbook 19th Edition
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
- 그 외
|
Copyright ⓒ 2015 John Sangwon Lee, MD, FAAP 미국 소아과 전문의, 한국 소아청소년과 전문의 이상원 저 “부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다. “The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.” |